20 / 10 / 16
医学翻译学习-肥厚型心肌病的临床病程和治疗
关于“肥厚型心肌病的临床病程和治疗”翻译学习,学习内容记录于此。
Clinical Course and Management of Hypertrophic Cardiomyopathy
肥厚型心肌病(HCM)是最常见的单基因心血管疾病,其表现和自然史多种多样,经常被误解,并且在临床实践中常常认识不足。
Hypertrophic cardiomyopathy (HCM), the most common monogenic cardiovascular disorder, is diverse in presentation and natural history, frequently misunderstood, and often underrecognized in clinical practice.
笔记:
- 肥厚型心肌病(HCM) hypertrophic cardiomyopathy
- 表现多样 be diverse in presentation
- 自然史 natural history
- 认识不足 underrecognized
55年前,美国国立卫生研究院的Braunwald研究组首次对HCM进行了全面的临床描述;当时HCM被称为特发性肥厚性主动脉瓣下狭窄。
A comprehensive clinical description of the disease was first made 55 years ago by the Braunwald group at the National Institutes of Health; at that time it was called idiopathic hypertrophic subaortic stenosis.
笔记:
- 特发性肥厚性主动脉瓣下狭窄 idiopathic hypertrophic subaortic stenosis
对各种HCM的诊断特征、遗传因素、临床病程和治疗的理解已经有了长足发展,特别是在过去的15年中。
An understanding of diagnostic features, genetic factors, clinical course, and management of the broad spectrum of HCM has evolved measurably, particularly in the past 15 years.
笔记:
- evolve 发展
已经出现了大量文献(超过18,000份报告),并且在许多方面,当代HCM与既往时代的HCM明显不同。
A vast literature (more than 18,000 reports) has emerged, and in many respects, contemporary HCM differs markedly from the disease of previous eras.
笔记:
- emerge
流行病学特征
Epidemiologic Features
诊断和患病率
Diagnosis and Prevalence
HCM的临床诊断是基于在没有其他心脏、全身性、代谢性或综合征性疾病的情况下,通过超声心动图或磁共振成像(MRI)识别出左心室肥大但未扩张。
Clinical diagnosis of HCM is based on a hypertrophied, nondilated left ventricle — which is identified by means of echocardiography or magnetic resonance imaging (MRI) — in the absence of another cardiac, systemic, metabolic, or syndromic disease.
笔记:
- 磁共振成像(MRI) magnetic resonance imaging
- in the absence of
基于超声心动图的流行病学研究显示,一般人群中HCM的患病率为1/500,但临床和基因诊断(包括在家人中做出的诊断)均考虑在内时,患病率较高(1/200)。
Echocardiography-based epidemiologic studies have shown a disease prevalence of 1 case per 500 persons in the general population but a higher prevalence (1 case per 200) when both clinical and genetic diagnoses, including those in family members, are taken into account (Fig. 1).
笔记:
- a disease prevalence of 1 case per 500 persons 患病率为1/500
在美国,估计750,000人可能患HCM。
An estimated 750,000 persons in the United States may be affected by HCM.
然而,仅其中的一小部分(约100,000人)被诊断患HCM,通常通过无创影像学检查诊断出患病,这提示大多数人在其一生中没有得到诊断。
However, the disease has been diagnosed in only a fraction of them (about 100,000), usually by means of noninvasive imaging, which suggests that most persons do not receive a diagnosis during their lifetime.
笔记:
noninvasive imaging 无创影像学检查
对HCM认识不足在女性和缺少医疗服务的少数群体中造成了与其人数不成比例的影响,有证据表明对黑种人的HCM认识不足,包括HCM未被诊断的男性黑种人死在运动场上,以及HCM黑种人患者可能较少被转诊接受HCM相关专业化治疗。
Underrecognition of HCM has disproportionately affected women and also underserved minorities, with evidence of underrecognition among blacks including deaths on the athletic field of black men with undiagnosed disease and potential underreferral of affected black patients for specialized HCM-related treatments.
笔记:
- 采取了顺译法
- 英文构句值得学习
- 中文后半段略显绕口,似乎可以拆句。且总论点先出,似不符合中文表达习惯
全球负担
Global Burden
已在122个国家(占世界人口的约90%)发现了HCM,自发(新生)突变很可能是造成疾病负担的原因。
HCM has been identified in 122 countries (representing approximately 90% of the world population), with spontaneous (de novo) mutations probably accounting for this disease burden (Fig. 1).
笔记:
- be identified
- de novo 新生
全世界可能约2,000万人患HCM,远超过最初认为的患病人数。
It is likely that HCM affects approximately 20 million people globally, well beyond the population that was initially thought to be affected.
HCM在许多国家、族群和人种中发生,并且男女患病率相同,而其临床表现和表型表达以及遗传基础似乎不随人口统计学特征的不同而发生明显变化。
Although the disease occurs in many countries, ethnic groups, and races and affects both sexes equally, its clinical and phenotypic expression and genetic substrate do not appear to vary substantially according to demographic characteristics.
笔记:
- clinical and phenotypic expression 临床表现和表型表达
在世界上许多地方,肥厚型心肌病未得到充分认识,但对该病的认识目前正渗入中国、印度和其他发展中国家的卫生系统,形成了诊断和治疗的新前沿。
Hypertrophic cardiomyopathy has been underrecognized in many parts of the world, but an awareness of the disease is now penetrating the health care systems in China, India, and other developing countries, defining an emerging frontier for diagnosis and management.
笔记:
- emerging frontier for diagnosis and management 诊断和治疗的新前沿
遗传因素
Genetic Factors
HCM以常染色体显性模式遗传,与心肌肌节或Z盘粗、细肌丝收缩结构蛋白的≥11个编码基因的突变(核苷酸序列变异体)相关,最常见的是β-肌球蛋白重链和肌球蛋白结合蛋白C基因的突变。
HCM is inherited in an autosomal dominant pattern, associated with mutations (nucleotide sequence variants) in 11 or more genes encoding proteins of thick and thin myofilament contractile components of the cardiac sarcomere or Z disk, with beta-myosin heavy chain and myosin-binding protein C genes most commonly involved.
笔记:
- inherited in an autosomal dominant pattern 以常染色体显性模式遗传
- with ··· most commonly involved 最常见的是···
基因检测显示本病存在巨大的异质性和不同的分子途径,已发现超过2,000种肌节突变。
Genetic testing panels show vast heterogeneity and diverse molecular pathways, with more than 2000 sarcomere mutations identified.
笔记:
- Genetic testing panel 中英文处理
一些突变被认为具有致病性,但其他突变的致病性不确定,并且许多突变仅限于单个家族(图1)。
Some of the mutations are considered to be pathogenic, but in others pathogenicity is uncertain, and many are confined to single families (Fig. 1).
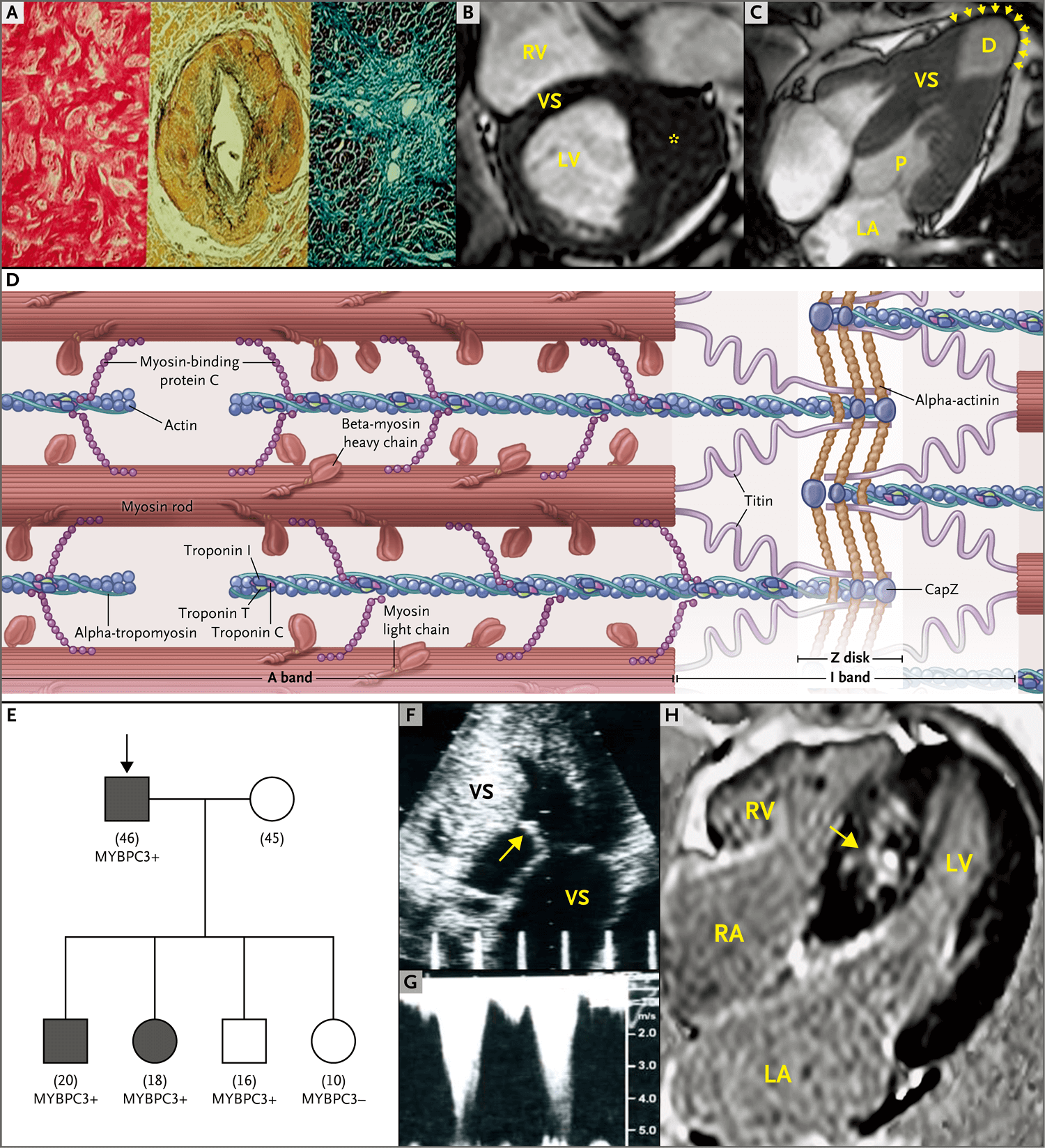
图1.肥厚型心肌病(HCM)的病理生理学基础
Figure 1. Pathophysiological Substrate of Hypertrophic Cardiomyopathy (HCM).
图A(苏木精和伊红)显示HCM的组织病理学特征:左心室(LV)心肌结构紊乱,相邻的肌细胞以垂直和倾斜角度排列(左),心肌壁内冠状动脉微动脉异常、动脉壁(动脉中层)增厚,管腔狭窄(中),可见心肌瘢痕(右)。
Panel A (hematoxylin and eosin) shows the histopathological features of HCM: disorganized architecture of the left ventricular (LV) myocardium with adjacent myocytes arranged at perpendicular and oblique angles (left), an abnormal intramural coronary arteriole with a thickened wall (media) and narrowed lumen (center), and a myocardial scar (right).
笔记:
- hematoxylin 苏木精
- eosin 伊红
- myocardial scar 心肌瘢痕
图B显示肥大局限于前外侧游离壁(星号),这是MRI可以最可靠显现的模式。
Panel B shows hypertrophy confined to the anterolateral free wall (asterisk), a pattern most reliably visualized on MRI.
RV表示右心室,VS表示室间隔。
RV denotes right ventricle, and VS ventricular septum.
图C显示薄壁心尖动脉瘤(箭头),这一发现与VS肥大相关,会增加任何年龄的猝死风险。
Panel C shows a thinwalled apical aneurysm (arrowheads), a finding associated with an increased risk of sudden death at any age in association with VS hypertrophy.
笔记:
- sudden death 猝死
D表示远端心腔,LA表示左心房,P表示近端心腔。
D denotes distal cavity, LA left atrium, and P proximal cavity.
图D中心肌肌节的图显示11个HCM肌节基因。
The diagram of a cardiac sarcomere in Panel D shows 11 HCM sarcomere genes.
图E显示具有肌球蛋白结合蛋白C(MBPC3)突变的HCM家族谱系。
Panel E shows an HCM family pedigree with a myosinbinding protein C (MBPC3) mutation.
笔记:
- HCM家族谱系 HCM family pedigree
父亲和四个孩子中的两个患HCM,一个孩子未患HCM,也未进行进一步临床检查,一个孩子有致病突变但无LV肥大。
The father and two of his children had HCM, another child was unaffected and was excluded from further clinical testing, and one child had a pathogenic mutation without LV hypertrophy.
黑色符号表示患HCM的家庭成员,白色符号表示未患HCM的家庭成员,正方形表示男性家庭成员,圆圈表示女性家庭成员;箭形表示先证者。
Black symbols denote affected family members, white symbols unaffected family members, squares male family members, and circles female family members; the arrow indicates the proband.
笔记:
- denote
符号下的数字表示检查时的年龄(岁)。
The numbers under the symbols indicate age (in years) at the time of testing.
图F和图G中的超声心动图来自同一患者。
The echocardiograms in Panels F and G are from the same patient.
笔记:
- 加粗用法值得注意
图F显示由于二尖瓣收缩期前移和间隔接触引起的LV流出道梗阻(箭形),而图G显示来自连续波多普勒检查的波形,其中主动脉下压力梯度估计约为100 mmHg。
Panel F shows LV outflow obstruction due to mitralvalve systolic anterior motion and septal contact (arrow), and Panel G shows waveforms from a continuouswave Doppler study, with a subaortic gradient estimated to be about 100 mm Hg.
笔记:
- LV outflow obstruction LV流出道梗阻
- subaortic gradient 主动脉下压力梯度
图H显示给予钆后的晚期增强区域(白色),这一发现与VS中的纤维化一致(箭形)。
Panel H shows areas of late enhancement (white) after the administration of gadolinium, a finding that is consistent with fibrosis in the VS (arrow).
RA表示右心房。
RA denotes right atrium.
由于这些开创性的见解,对于未通过其他方式知晓遗传患病状态的患者,能够根据实验室检查诊断HCM。
These seminal insights have made it possible to diagnose HCM on the basis of laboratory testing in patients who otherwise would be unaware of their genetically affected status.
笔记:
-
seminal
(formal) very important and having a strong influence on later developments (对以后的发展)影响深远的,有重大意义的
-
由于···,对于···,能;这一句似乎为无主语病句。
然而,基因型-表型相关性不一致,并且单个(或多个)肌节变异体在预测预后方面不可靠,在风险分层中没有特异的作用。
However, genotype–phenotype correlations have been inconsistent, and single (or multiple) sarcomere variants are unreliable in predicting prognosis, with no specific role in risk stratification.
笔记:
- genotype–phenotype correlations 基因型-表型相关性
- be unreliable in v-ing
因此,HCM的重要治疗决策完全基于临床标准。
Thus, important management decisions in cases of HCM are based solely on clinical criteria.
笔记:
- 完全基于 be based solely on
基因检测主要局限于下一代(级联)家庭筛查,这有机会识别不太可能遗传HCM的家庭成员,以及无左心室肥大的患HCM家庭成员(图1)。
Genetic testing is confined largely to next-generation (cascade) family screening, which affords the opportunity to identify family members who are unlikely to inherit HCM, as well as affected family members without left ventricular hypertrophy (Fig. 1).
笔记:
- afford the opportunity to 有机会···
这些突变基因携带者在特征上无心脏事件或症状,并且许多携带者永远不会罹患HCM,但是仍然可以将致病突变传递给后代。
Such gene carriers characteristically have no cardiac events or symptoms, and many carriers will never have HCM but can nevertheless transmit disease-causing mutations to subsequent generations.
笔记:
disease-causing mutations 致病突变
基因检测还可以识别类似HCM的代谢和蓄积拟表型(例如溶酶体相关膜蛋白2 [LAMP2]心肌病、法布里病[Fabry’s disease]、PRKAG2和淀粉样变性)。
Genetic testing can also identify metabolic and storage phenocopies (e.g., lysosome-associated membrane protein 2 [LAMP2] cardiomyopathy, Fabry’s disease, PRKAG2, and amyloidosis) that mimic HCM.
笔记:
- metabolic and storage phenocopies 代谢和蓄积拟表型
随着技术进步(全基因组测序),意义不确定的变异体变得越来越多,这使得对致病性的解释变得越来越复杂,并且可能导致在不同的人种、族群和家系人群中,将良性变异体错误解释为具有致病性。
With technological advances (whole-genome sequencing), variants of uncertain significance have become more numerous, making interpretation of pathogenicity increasingly complex and potentially leading to misinterpretation of benign variants as pathogenic in diverse racial, ethnic, and ancestry populations.
笔记:
- whole-genome sequencing 全基因组测序
实际上,目前仅1/3的HCM先证者具有适合家庭筛查的致病性(或很可能致病的)突变。
Indeed, at present, only one third of probands with HCM have pathogenic (or probably pathogenic) mutations suitable for family screening.
笔记:
- probands
散发性(非家族性)HCM(即无HCM家族史的患者出现肌节突变)可能比目前认为的更常见。
Sporadic (nonfamilial) HCM (i.e., sarcomere mutations in a patient without a family history of HCM) may be more common than currently thought.
影像学检查中的形态特征
Morphologic Features on Imaging Studies
左心室肥大
Left Ventricular Hypertrophy
HCM表型特征的确定是基于近50年的超声心动图成像。
Characterization of the HCM phenotype has been based on almost 50 years of echocardiographic imaging.
高分辨率断层扫描MRI可以对一些患者的左心室肥厚做出更可靠的评估,并通过体内识别心肌纤维化,加强风险分层(图1)。
High-resolution tomographic MRI can provide a more reliable assessment of left ventricular hypertrophy in some patients, as well as enhanced risk stratification through in vivo identification of myocardial fibrosis (Fig. 2).
笔记:
- High-resolution tomographic MRI 高分辨率断层扫描MRI
临床诊断的大多数病例左心室壁厚度≥15 mm(平均21 mm),但有时会非常厚(30~50 mm)。
In most clinically diagnosed cases, left ventricular wall thickness is 15 mm or more (average, 21 mm), but there is massive thickness (30 to 50 mm) in some cases.
笔记:
- average, xx
- massive thickness
临界性厚度(13~14 mm)通常需要与全身性高血压或生理性运动员心脏进行鉴别诊断(图1)。
Borderline thickness (13 to 14 mm) often requires differential diagnosis from systemic hypertension or physiologic athlete’s heart (Fig. 1).
笔记:
- borderline thickness 临界性厚度
运动员心脏是指多数时候每天接受训练>1小时的人的心脏所发生的结构和功能的改变。此改变无症状,体征包括心动过缓、收缩期杂音和额外心音。心电图异常常见。根据临床表现或超声心动图诊断。无需治疗。运动员心脏值得注意,它必须同严重心脏疾病相鉴别。
然而,左心室壁的任何厚度均与HCM的临床表现一致,包括突变基因携带者的正常尺寸。
However, any left ventricular wall thickness is consistent with the clinical spectrum of HCM, including normal dimensions in gene carriers.
左心室厚度增加与猝死风险增加相关,但不一定与心力衰竭进展相关。
Greater left ventricular thickness is associated with an increased risk of sudden death but not necessarily of progression to heart failure.
表型表达包括无数非常多变的不对称肥大模式,即使在一级亲属中也是如此。
Phenotype expression includes a myriad of asymmetric patterns of hypertrophy that are highly variable even among first-degree relatives.
笔记:
一级亲属是一个人的父母、子女以及兄弟姐妹(同父母)。
二级亲属,一个人和他的叔、伯、姑、舅、姨、祖父母、外祖父母。
三级亲属,表兄妹或堂兄妹。
另外还有一个直系亲属和旁系亲属的概念。
直系亲属是指配偶、父母(公婆、岳父母)、子女及其配偶、祖父母、外祖父母、孙子女(外孙子女)及其配偶、曾祖父母、曾外祖父母。
旁系亲属就是指除了直系血亲之外与自己有共同祖先的亲属就是旁系亲属关系。比如兄弟姐妹之间、姑侄之间都是。
这些模式可以是弥漫性、节段性(包括心尖的)、局灶性或者不连续或病灶延伸到右心室,以及存在细长的二尖瓣小叶或充满血液的隐窝。
These patterns can be diffuse, segmental (including apical), focal, or noncontiguous or could involve extension into the right ventricle, as well as elongated mitral leaflets or blood-filled crypts.
因为左心室肥大通常发生在青春期和加速生长期,所以初始家庭筛查的首选方案是从12~21岁开始,每12~18个月进行1次诊断性成像检查,虽然中断临床病程的不良事件罕见(图1)。
The preferred option for initial family screening is diagnostic imaging every 12 to 18 months from the ages of 12 to 21 years, given that left ventricular hypertrophy commonly develops during adolescence and periods of accelerated growth, although adverse events punctuating the clinical course are rare (Fig. 1).
笔记:
- 诊断性成像检查 diagnostic imaging
- 英文构句顺序
由于表型可能延迟到中年出现,因此有理由以5年的间隔期进行长期影像学监测。
The possibility of delayed penetrance of the phenotype into midlife can justify extended imaging surveillance at 5-year intervals.
采用脉冲和组织多普勒、应变率成像和数字斑点追踪进行的超声心动图评估,使得我们能够了解舒张功能障碍、总体和局部心肌力学以及收缩期射血决定因素的机械和功能信息。
Echocardiographic assessment with pulsed and tissue Doppler, strain rate imaging, and digital speckle tracking has provided mechanistic and functional insights into diastolic dysfunction, global and regional myocardial mechanics, and determinants of systolic ejection.
然而,这些措施尚未显著影响HCM预后或治疗。
However, these initiatives have not yet substantially affected disease prognosis or management.
流出道梗阻
Outflow Obstruction
HCM主要是一种梗阻性疾病,70%的患者在休息或生理性激发(即运动)时对左心室流出产生机械阻力(梯度≥30 mmHg)(图1)。
HCM is predominantly an obstructive disease, with 70% of patients having mechanical impedance to left ventricular outflow (gradients ≥30 mm Hg) at rest or with physiological provocation (i.e., exercise) (Fig. 2).
主动脉下压力梯度具有动态特征,随着生理负荷条件(例如,由于脱水、摄入酒精或食物或者从坐位变为站立位,心室容积缩小,主动脉下压力梯度增加)而变化,这些变化常常是症状日常波动的原因。
Subaortic gradients are characteristically dynamic and subject to change with physiological loading conditions (e.g., increased with reduced ventricular volume due to dehydration, alcohol or food consumption, or a change from a sitting to a standing position), and these changes are often responsible for daily fluctuations in symptoms.
笔记:
- characteristically
- a change from a sitting to a standing position 从坐位变为站立位
- daily fluctuations 日常波动
流出道梗阻通常由二尖瓣收缩期前移和因流动阻力导致的间隔接触造成,还会导致二尖瓣反流(图1)。
Outflow obstruction is usually produced by mitral-valve systolic anterior motion and septal contact due to flow drag, also resulting in mitral regurgitation (Fig. 1).
笔记:
- be produced by
- anterior motion 前移
- septal contact 间隔接触
- flow drag 流动阻力
乳头肌先天性直接异常插入二尖瓣(中间无腱索)偶尔会导致心室中部肌肉性梗阻,并且与计划实施侵入性治疗策略相关。
Congenital, anomalous insertion of the papillary muscle directly into the mitral valve (without interposition of chordae) is occasionally responsible for midventricular muscular obstruction and is relevant to the planning of invasive treatment strategies.
笔记:
- invasive treatment strategies 侵入性治疗策略
临床病程和治疗
Clinical Course and Management
HCM的临床病程主要是根据来自三级转诊中心的观察数据进行定义,其特征多样(图2和图3)。
The clinical course of HCM, defined primarily on the basis of observational data from tertiary referral centers, is characteristically diverse (Figs. 3 and 4).
笔记:
- Figs. 3 and 4,多图表示,可Figs. (另有规定除外)
- tertiary referral center 三级转诊中心
许多患者没有临床上显著的症状和不良事件,不需要接受主要的治疗干预,并且寿命正常或长寿。
Many patients remain free of clinically significant symptoms and adverse events, do not require major treatment interventions, and have normal or extended longevity.
笔记:
- free of xxx
这类患者越来越多地被偶然发现,通常疾病表现为轻度。
Increasingly, such patients are identified fortuitously, usually with mild disease expression.
在其他患者中,HCM沿着特定的疾病途径发展,被改变疾病自然史的临床事件中断,必须采用针对性的有效治疗策略(图3)。
In other patients, HCM progresses along specific disease pathways, punctuated by clinical events that alter the natural history of the disease and dictate targeted and effective treatment strategies (Fig. 4).
**
图2. HCM患者的风险分层和使用植入式心律转复除颤器(ICD)对猝死的一级预防
Figure 2. Risk Stratification and Primary Prevention of Sudden Death with Implantable Cardioverter–Defibrillators (ICDs) in Patients with HCM.
笔记:
- primary prevention 一级预防
- 中文中的“使用”为增译
预防性ICD植入术的患者选择是基于风险的主要标志,有时与潜在的风险调节因素相关。
Selection of patients for prophylactic ICD placement is based on major markers of risk, sometimes in association with potential risk mediators.
阳性家族史通常定义为因HCM猝死的一级亲属。
A positive family history is usually defined as a first-degree relative who died suddenly from HCM.
MRI上广泛的晚期钆增强(LGE)(≥15%的LV质量)表明弥漫性纤维化,是该列表中的新增内容。
Extensive late gadolinium enhancement (LGE) (≥15% of LV mass) on MRI indicates diffuse fibrosis and is a recent addition to the list.
笔记:
- 英文原文为“主+v1+v2”结构,中文似乎有歧义。
LV心尖动脉瘤需要考虑将除颤器疗法作为一级预防(不论动脉瘤大小或患者年龄如何),并且不是手术的主要适应证。
An LV apical aneurysm warrants consideration of defibrillator therapy as primary prevention, regardless of the size of the aneurysm or the patient’s age, and is not a primary indication for surgery.
笔记:
- warrant:(formal) to make sth necessary or appropriate in a particular situation 使有必要;使正当;使恰当
- regardless of
- 译文似乎太过于贴近原文。实则无中文内涵。
在接受室间隔酒精消融术的患者亚组中,用于预防猝死的风险分层策略尚未解决。
Risk stratification for the prevention of sudden death in the subgroup of patients who undergo alcohol septal ablation has not been resolved.
笔记:
- “策略”为增译
按照惯例,等待心脏移植的患者接受ICD干预。
By convention, patients awaiting heart transplantation receive ICDs.
笔记:
- By convention 按照惯例
心脏停搏后的复苏是使用植入式除颤器进行二级预防的明确适应证。
Resuscitation after cardiac arrest is an unequivocal indication for secondary prevention with an implantable defibrillator.
- unequivocal indication 明确适应证
接受过ICD干预的HCM患者随后发生心力衰竭或死亡的风险较低(每年<1%);相比之下,在缺血性心脏病患者中,接受ICD干预后1年时的死亡风险为20%,需要住院治疗的心力衰竭风险为30% 。
Patients with HCM who have had an ICD intervention subsequently have a low risk of heart failure or death (<1% per year); in contrast, the risk of death 1 year after an ICD intervention in patients with ischemic heart disease is 20%, with a 30% risk of heart failure requiring hospitalization.
LVH表示左心室肥大,NSVT表示非持久性室性心动过速(动态心电图监测),VT表示室性心动过速,VF表示心室颤动。
LVH denotes left ventricular hypertrophy, NSVT nonsustained ventricular tachycardia (on ambulatory monitoring), VT ventricular tachycardia, and VF ventricular fibrillation.

图3. HCM临床表现的治疗流程
Figure 3. Management Algorithm for the Clinical Spectrum of HCM.
除移植外,非梗阻性HCM患者晚期心力衰竭(HF)的治疗包括心脏活性药物、心脏再同步治疗和LV辅助装置。SD表示猝死。
In addition to transplantation, treatments for advanced heart failure (HF) in patients with nonobstructive HCM include cardioactive drugs, cardiac-resynchronization therapy, and LV-assist devices. SD denotes sudden death.
猝死
Sudden Death
HCM最初是在猝死的背景下描述的,猝死仍然是本病在有或无梗阻的患者中最明显的并发症(图3),特别是考虑到媒体对竞技运动员心脏停搏的报道。
HCM was initially described in the context of sudden death, which remains the most visible complication of the disease in patients with or without obstruction (Fig. 4), especially given media coverage of cardiac arrests in competitive athletes.
在室性心动过速导致的猝死中,对于无法预测的致心律失常的基础,我们通过以下组织病理学标志确定:心肌结构紊乱,间质胶原沉积,以及冠状微血管介导血流功能障碍和缺血,进而导致心肌细胞死亡后形成的替代瘢痕(图1)。
In cases of sudden death due to ventricular tachyarrhythmias, the unpredictable arrhythmogenic substrate is defined by the histopathological hallmarks of disorganized myocardial architecture, interstitial collagen deposition, and replacement scarring after myocyte death as a consequence of coronary microvascularmediated flow dysfunction and ischemia (Fig. 1).
笔记:
“基础”和substrate?
根据美国心脏病学会(American College of Cardiology)和美国心脏学会(American Heart Association)(ACC-AHA)出版的共识治疗指南以及较新数据,已将若干临床标志整合到风险分层流程中。
Several clinical markers have been assembled into a risk-stratification algorithm in accordance with consensus management guidelines (U.S. and Canadian) published by the American College of Cardiology and the American Heart Association (ACC–AHA)6 and more recent data.
笔记:
- be assembled into 整合
对于后续除颤器干预能够可靠终止室性心动过速和心室颤动的大部分猝死高危患者,这一策略能够高效且灵敏地予以识别。
This strategy has been highly effective and sensitive for identifying the vast majority of individual patients at increased risk for sudden death, in whom subsequent device therapy reliably terminates ventricular tachycardia and fibrillation.
对于临床表现中有一种或多种常规危险因素被判定为显著的年轻患者和中年患者,应考虑预防性植入除颤器(图2)。
Prophylactic defibrillator placement should be considered for young and middle-aged patients whose clinical profiles include one or more conventional risk factors judged to be major (Fig. 2).
笔记:
- clinical profile
根据病史、影像学检查和动态心电图(ECG)监测,最重要的已证实的风险标志是不明原因的晕厥、极端的左心室壁厚度、一级亲属的HCM相关猝死,以及非持续性室性心动过速的多次或长期发作。
On the basis of the history taking, imaging studies, and ambulatory electrocardiographic (ECG) monitoring, the most important established risk markers are unexplained syncope, extreme left ventricular wall thickness, HCM-related sudden death in a first-degree relative, and multiple or prolonged episodes of nonsustained ventricular tachycardia.
以下两项已被加入HCM风险分层流程中:左心室心尖动脉瘤伴有局部瘢痕,以及MRI晚期钆增强可见的广泛心肌纤维化(图1和图2)。
Left ventricular apical aneurysm with regional scarring, as well as extensive myocardial fibrosis seen as late gadolinium enhancement on MRI, has been added to the risk-stratification algorithm for HCM (Figs. 1 and 2).
笔记:
- regional scarring 局部瘢痕
如果风险水平仍不确定,其他临床特征(例如左心室流出道梗阻)可作为风险调节因素,并共同制订决策(图2)。
If the level of risk remains uncertain, other clinical features such as left ventricular outflow obstruction can serve as mediating factors in association with shared decision making (Fig. 2).
笔记:
- mediating factors 调节因素
- 中文有病句倾向
自相矛盾的是,年龄≥60岁的HCM患者(即使是有风险标志的患者)基本上不会发生猝死(发生率每年0.2%,这与一般人群的猝死发生率相似)(图2)。
Paradoxically, patients with HCM who survive into the seventh decade and beyond, even those with risk markers, are largely protected from sudden death (rate, 0.2% per year, which is similar to the rate in the general population) (Fig. 3).
对于这些患者,要根据每例患者的具体情况决定是否预防性植入除颤器。
Decisions about prophylactic defibrillator placement in such patients are made on a case-by-case basis.
笔记:
- a case-by-case basis 具体情况
值得注意的是,少数无风险标志的患者可能会发生致死性心律失常事件,这强调了扩大风险分层的重要性。
It is notable that a small minority of patients without risk markers can nevertheless have fatal arrhythmic events, which underscores the importance of expanding risk stratification.
HCM是美国运动场猝死的最重要原因。
HCM is the most important cause of sudden death on the athletic field in the United States.
激烈的竞技运动是一个主要的风险标志,因此对于患HCM的年轻学生运动员,谨慎地取消其参加此类活动的资格是合理的。
Intense competitive sports represent a primary risk marker that can justify prudent disqualification of young student athletes with HCM from such activities.
然而,适度的非竞技性休闲运动可以接受,因为没有证据表明休闲运动会增加对重要快速性心律失常的易感性,而且在美国,无左心室肥大但遗传上受累的人不会被取消参加竞技运动的资格。
However, a moderate level of noncompetitive, recreational exercise is acceptable, since there is no evidence that it increases susceptibility to important tachyarrhythmias, and genetically affected persons without left ventricular hypertrophy are not disqualified from competitive sports in the United States.
各种异常心电图模式(存在于多达90%的患者中)不能预测临床病程,但可能代表HCM后续发展的诊断标志物。 A variety of abnormal ECG patterns (present in up to 90% of patients) do not predict the clinical course but may represent diagnostic markers for the subsequent development of HCM.
欧洲HCM指南已经在推广可通过在线计算器计算的猝死风险评分。
A sudden-death risk score, accessible with an online calculator, has been promoted by the European HCM guidelines.
然而,当应用于个体HCM患者时,对于放置置入式心律转复除颤器(ICD)的临床决策,风险评分的敏感性较低,对无ICD干预情况下未受保护且易发生猝死的高危患者识别不足。
However, when applied to individual patients with HCM, the risk score has low sensitivity for making clinically relevant decisions about implantable cardioverter–defibrillator (ICD) placement, significantly underidentifying high-risk patients who would remain unprotected and susceptible to sudden death without ICD therapy.
在过去的15年中,经静脉ICD取代了药物治疗策略,并使成人和儿童HCM患者猝死的预防成为现实,改变了许多患者的临床病程(图3)。
During the past 15 years, transvenous ICDs have taken the place of pharmacologic strategies and have made the prevention of sudden death a reality for both adults and children with HCM, altering the clinical course for many patients (Fig. 3).
笔记:
- take place of
- pharmacologic strategies
- make sth. a reality ···
这一治疗范例基于来自多项大型多中心和国际性高危患者登记系统的一致数据。
This management paradigm is based on consistent data from a number of large multicenterd international high-risk registries.
除颤器干预能够有效地终止室性心动过速或心室颤动(这些事件最常发生在中年);对基于临床风险标志的一级预防,需要除颤器干预的室性心动过速或心室颤动的平均年发生率为4%,对心脏停搏后的二级预防,平均年发生率为10% (图2),但许多接受ICD植入的患者可能最终未接受过ICD干预。
Defibrillator interventions effectively terminate ventricular tachycardia or fibrillation — with these events occurring most often in midlife — at an average rate of 4% per year for primary prevention based on clinical risk markers and at a rate of 10% per year for secondary prevention after cardiac arrest (Fig. 3), although many patients receiving ICDs may not ultimately have device therapy.
ICD干预的时间无法预测,已有植入和干预之间间隔10~15年的报告。
The timing of ICD interventions can be unpredictable, and intervals of 10 to 15 years have been reported between implantation and intervention.
笔记:
- timing
- interval
- report v. 报告 n.
与缺血性心脏病患者的ICD干预不同,HCM患者的ICD干预与随后的临床恶化(包括心力衰竭和肾功能障碍导致的死亡)无关(图2)。
Unlike ICD interventions in patients with ischemic heart disease, device interventions in patients with HCM are not associated with subsequent clinical deterioration, including death from heart failure and renal dysfunction (Fig. 3).
笔记:
这一句话的英文很经典。
- Unlike vs. Different from
- in vs. for
- device interventions 体现了英文的多变化
- from,而没有用due to, caused by 等
调查显示,接受除颤器治疗的HCM患者报告焦虑和抑郁水平较低,可以接受。
Surveys show that patients with HCM who undergo treatment with defibrillators report acceptably low levels of anxiety and depression.
植入除颤器的决定需要考虑除颤器并发症的发生率(每年3%~5%),最常见的是由于室上性或窦性心动过速和导线断裂引起的不适当的电击。
The decision to implant a defibrillator requires consideration of the rate of device complications (3 to 5% per year) — most frequently, inappropriate shocks due to supraventricular or sinus tachycardia and lead fractures.
笔记:
- the decision to do sth. requires consideration of/that
皮下除颤器具有潜在的优势,特别是能够保护年轻患者的静脉系统和避免长期导线并发症,但这种除颤器在HCM患者中终止自发性心室颤动的疗效仍不清楚。
Subcutaneous defibrillators have potential advantages, particularly protection of the venous system in younger patients and avoidance of long-term lead complications, although the efficacy of such defibrillators in aborting spontaneous ventricular fibrillation in patients with HCM remains unclear.
笔记:
- 名词简短插入语,规避了过于复杂的从句。
心力衰竭
Heart Failure
大部分HCM患者有轻至重度功能损害,通常表现为劳力性呼吸困难和疲劳(伴或不伴胸痛);端坐呼吸和阵发性夜间呼吸困难不常见。
A large proportion of patients with HCM have mild-to-severe functional impairment, usually expressed as exertional dyspnea and fatigue (with or without chest pain); orthopnea and paroxysmal nocturnal dyspnea are uncommon.
临床队列中女性的比例不足,但与男性相比,女性就诊时的年龄往往较大(并且诊断较晚),且症状较严重,心肺运动表现受损程度较大。
Women are underrepresented in clinical cohorts but on presentation tend to be older than men (and with a delayed diagnosis) and have more severe symptoms, with greater impairment in cardiopulmonary exercise performance.
尽管如此,男性和女性的HCM死亡率(包括猝死率)无显著差异。
Nevertheless, men and women do not differ significantly with respect to the rate of death from HCM, including sudden death.
笔记:
-
A and B (do not) differ with respect to FIELD
心力衰竭和流出道梗阻
Heart Failure and Outflow Obstruction
在心力衰竭导致慢性、药物难治性失能的患者中,90%患者的主要原因是左心室流出道梗阻(静息或运动时),导致左心室压力显著升高和继发性二尖瓣反流。
For 90% of patients with chronic, drug-refractory disability from heart failure, the primary cause is left ventricular outflow obstruction (at rest or with exercise), which leads to markedly elevated left ventricular pressures and secondary mitral regurgitation.
HCM患者的心力衰竭常伴有肺动脉高压、舒张功能障碍、运动时每搏输出量不增加,并且可能因外在因素(例如肥胖)而恶化(图3)。
Heart failure in patients with HCM is often accompanied by pulmonary hypertension, diastolic dysfunction, and absence of an increase in stroke volume with exercise and is potentially exacerbated by extrinsic factors (e.g., obesity) (Fig. 3).
静息时主动脉下压力梯度导致进行性心力衰竭的年发生率约为5%,虽然自相矛盾,但一些压力梯度较大的患者几乎长期无症状,有时甚至到高龄时仍未出现症状。
The rate at which subaortic gradients at rest lead to progressive heart failure is about 5% per year, although paradoxically, some patients have large gradients with little or no symptoms over long periods of time, sometimes even to an advanced age.
药物治疗是梗阻性HCM患者的首选疗法和治疗的基石。
Pharmacologic therapy is the first option and the mainstay of treatment in patients with obstructive HCM.
- 笔记: Pharmacologic therapy 药物治疗
许多此类患者对药物治疗有良好反应,症状得到控制,生活质量恢复,疗效持续时间不同。
Many such patients have a favorable response to pharmacologic therapy, with symptom control and a restored quality of life for varying periods of time.
笔记:
- a favorable response to xxx 对xxx有良好反应
用于缓解梗阻性HCM患者的心力衰竭、胸痛或这两种症状的心脏活性药物传统上包括房室结阻滞剂和丙吡胺;30多年来,尚未引入其他HCM治疗药物。
Cardioactive medications administered to mitigate symptoms of heart failure, chest pain, or both in patients with obstructive HCM traditionally include atrioventricular nodal blocking agents and disopyramide; additional drugs for the treatment of HCM have not been introduced in more than 30 years.
β肾上腺素能受体阻滞剂(阿替洛尔、美托洛尔和普萘洛尔)和钙通道阻滞剂(维拉帕米和地尔硫䓬)对静息压力梯度具有不一致的效应,但运动激发的梗阻可使用β受体阻滞剂抑制交感神经刺激,进而减轻梗阻。
Beta-adrenergic blocking agents (atenolol, metoprolol, and propranolol) and calcium-channel blockers (verapamil and diltiazem) have inconsistent effects on the resting gradient, although exercise-provoked obstruction can be blunted by inhibiting sympathetic stimuli with beta-blockers.
丙吡胺(与β受体阻滞剂联合用药)的负性肌力作用可以在很长一段时间内减轻某些患者的静息压力梯度和症状。
The negative inotropic properties of disopyramide (administered with a beta-blocker) can reduce resting gradients and symptoms in some patients for substantial periods of time.
笔记:
- negative inotropic properties 负性肌力作用
- substantial periods of time 很长一段时间内
虽然对左心室流出道的机械阻力采取药物治疗可以引起不同程度的症状缓解,但几乎没有证据表明单独药物治疗能够从根本上长期改变HCM的自然史,或者能够引起左心室重塑。
Although pharmacologic treatment for mechanical impedance to left ventricular outflow can result in variable degrees of symptom relief, there is little evidence that drug therapy alone fundamentally alters the natural history of HCM over the long term or is responsible for left ventricular remodeling.
笔记:
- 机械阻力 mechanical impedance to
对于长期左心室流出道梗阻(静息或生理激发时,压力梯度≥50 mmHg)导致失能症状或生活质量受损的患(一般与纽约心脏学会分级中的Ⅲ级或Ⅳ级相符),适合接受一期经主动脉室间隔心肌切除术,或者特定患者适合接受室间隔酒精消融术,这种手术最适合按照ACC-AHA共识指南,在手术量大的多学科HCM中心实施(图3)。
Patients with disabling symptoms and an impaired quality of life (generally consistent with New York Heart Association class III or IV) due to long-standing left ventricular outflow obstruction at rest or with physiological provocation (gradient, ≥50 mm Hg) are candidates for primary transaortic septal myectomy or, in selected patients, alcohol septal ablation, most appropriately performed in high-volume, multidisciplinary HCM centers in accordance with ACC–AHA consensus guidelines (Fig. 3).
重度症状较少的特定患者被认为适合在手术量大的手术中心接受心肌切除术。
Selected patients with less severe symptoms have been considered candidates for myectomy performed in high-volume surgical centers.
笔记:
be considered candidates for ···
包括心肌切除术在内的侵入性治疗选项建议通常是基于对生活质量产生不良影响的劳力性呼吸困难的个人史,但当病史评估不确定时,心肺运动试验有助于阐明功能限制的程度。
Recommendations for invasive treatment options, including myectomy, are usually based on a personal history of exertional dyspnea that adversely affects quality of life, although cardiopulmonary exercise testing is useful in clarifying the degree of functional limitation when historical assessment is uncertain.
虽然已经使用了许多传统的,而主要是非生理性的策略(例如亚硝酸戊酯吸入、瓦氏[Valsalva]动作和异丙肾上腺素输入),但为了排除或识别其他的手术候选者,运动(应激)超声心动图是产生左心室流出道压力梯度(当静息时无压力梯度时)的首选方法(图3)。
Although a number of traditional, but largely nonphysiological strategies (e.g., amyl nitrite inhalation, the Valsalva maneuver, and isoproterenol infusion) have been used, exercise (stress) echocardiography is the preferred method to provoke left ventricular outflow gradients (when absent at rest), for the purpose of excluding or identifying additional surgical candidates (Fig. 3).
用于消除压力梯度和二尖瓣反流的扩大心肌切除术包括从室间隔基底部(可能有各种不同厚度)切除心肌,该手术常伴有二尖瓣重塑;可通过折叠术减少松弛和活动,重建二尖瓣下的心室结构,或者同时进行这两种手术。
Extended myectomy, performed to abolish the gradient and mitral regurgitation, involves muscular resection from the basal ventricular septum (which can range widely in thickness), frequently accompanied by remodeling of the mitral valve with plication to decrease slack and mobility, reconstruction of submitral intraventricular structures, or both.
在儿童和成人(平均年龄45~50岁)中均成功进行了心肌切除术,现在心肌切除术已成为最安全的心内直视手术之一,在手术量大的梗阻性HCM治疗中心,手术死亡率为0.4%,相对于35年前的手术死亡率降低了95%。
Myectomy has been performed successfully in both children and adults (average age, 45 to 50 years) and is now established as one of the safest open-heart procedures, with an operative mortality of 0.4% in centers with a high volume of obstructive HCM cases, representing a 95% reduction in mortality from 35 years ago.
在手术量较小的梗阻性HCM治疗中心进行心肌手术时,手术死亡的风险增加11倍。
The risk of operative death is increased by a factor of 12 when myectomy is performed in centers with a lower volume of such cases.
笔记:
增加n倍,increased by a factor of n+1
心肌切除术消除主动脉下压力梯度并使左心室压力和肺动脉压变为正常,因而永久地逆转了心力衰竭症状(不论之前症状持续多长时间),恢复了90%~95%患者的生活质量,包括70%以上患者的症状完全消失。
By abolishing subaortic gradients and normalizing left ventricular and pulmonary arterial pressures, myectomy permanently reverses symptoms of heart failure (regardless of their prior duration), restoring quality of life in 90 to 95% of patients, including more than 70% who become completely asymptomatic.
此外,心肌切除术的相关远期生存结局与一般人群相当,包括猝死风险可能下降。
In addition, myectomy is associated with long-term survival equivalent to that in the general population, including a possible reduction in the risk of sudden death.
在压力梯度消除后,症状未缓解不常见,通常与共存的损害、导致术后收缩或舒张功能障碍的严重心肌肥大或持续心房颤动相关。
Lack of symptomatic relief after the gradient is abolished is uncommon but is usually associated with compromising coexisting conditions, massive hypertrophy leading to postoperative systolic or diastolic dysfunction, or persistent atrial fibrillation.
外科手术的发展推动心肌切除术在更多地区得到应用,包括在印度和中国以及欧洲(在欧洲,这种手术未被充分利用)。
The progress in surgical management has provided an impetus to expand access to myectomy, including in India and China, as well as in Europe, where this operation has been underused.
根据ACC-AHA和欧洲共识指南,心肌超声造影下经皮酒精消融术已经成为心肌切除术的主要替代疗法。
On the basis of ACC–AHA and European consensus guidelines, percutaneous alcohol ablation with myocardial contrast echocardiography has become the primary alternative to myectomy.
酒精消融术的优点是侵入性较小,需要的住院时间较短。
Alcohol ablation has the advantages of being a less invasive procedure and requiring a shorter hospital stay.
这种手术通常用于不适合心肌切除术(由于共存疾病或手术动机不足)、不需要冠状动脉旁路移植术或瓣膜置换术、具有药物疗法难治性重度症状的特定高龄患者。
This procedure is usually reserved for selected patients of advanced age with severe symptoms that are refractory to drug therapy who are not candidates for myectomy (because of coexisting conditions or insufficient motivation for surgery) and who do not require coronary-artery bypass grafting or valve replacement.
靶向(医源性)、酒精诱导的透壁梗死能够使间隔基底部变薄、流出道扩大,进而模拟心肌切除术对压力梯度和症状产生的效应,但接受酒精消融术的患者中,有10%因心脏传导阻滞需要起搏器治疗;在因间隔瘢痕而易受损害的患者中,心律失常负担可能会增加。
The targeted (iatrogenic), alcohol-induced transmural infarct mimics the effects of myectomy on gradient and symptoms by virtue of basal septal thinning and outflow-tract enlargement, although 10% of patients who undergo alcohol ablation require a pacemaker for heart block; the arrhythmic burden may be increased in vulnerable patients because of septal scarring.
10%的患者需要重复消融,左心室流出道和间隔穿支动脉的不良解剖可能会限制疗效。
Ten percent of patients require repeat ablation, and unfavorable anatomy of the left ventricular outflow tract and septal perforator artery may limit treatment efficacy.
成功的室间隔酒精消融术依赖于多学科HCM中心较大的手术量和技术专长、适当的患者选择、对最小有效酒精剂量和梗死面积的强调,以及与基于导管的其他疗法相似的强制报告。
Successful alcohol septal ablation depends on high operator volume and technical expertise in a multidisciplinary HCM center, with appropriate patient selection, an emphasis on the minimal effective alcohol dose and infarct size, and mandatory reporting similar to that for other catheterbased therapies.
在符合这些标准的中心,手术死亡率可以低至1%,生存率与心肌切除术的生存率相似。
At centers that meet these criteria, procedural mortality can be as low as 1%, with survival rates that are similar to those for myectomy.
无梗阻的心力衰竭
Heart Failure without Obstruction
静息和运动时均不能产生流出道压力梯度的患者(即非梗阻性HCM患者)在转诊至专业HCM治疗中心的患者中占1/3。
Patients without the capacity to generate outflow gradients both at rest and with exercise (i.e., those with nonobstructive HCM) account for one third of patients referred to centers that specialize in the treatment of HCM.
这些患者病情基本上稳定,通常保留收缩功能,仅有轻度心力衰竭症状或无心力衰竭症状,并且一般预后良好。
Such patients are largely in stable condition, usually with preserved systolic function, only mild heart failure symptoms or none, and a generally favorable prognosis.
心脏活性药物(主要是β受体阻滞剂和维拉帕米)对其中相当大一部分患者的症状具有持续时间不同的有益作用。
Cardioactive drugs (primarily beta-blockers and verapamil) have beneficial effects on symptoms in a substantial proportion of these patients over variable periods of time.
劳力性呼吸困难很可能是由舒张功能障碍伴松弛和充盈受限或生理限制引起,虽然超声心动图指标可能无法可靠地反映这些异常血流动力学特征。
Exertional dyspnea is probably due to diastolic dysfunction with impaired relaxation and filling or restrictive physiology, although echocardiographic indexes may not reliably reflect these abnormal hemodynamic features.
笔记:
- be due to
在静息或生理激发时无梗阻的患者中,少数(约10%)患最强药物治疗方案难治的进展性终末期心力衰竭,最终可能需要接受心脏移植(图3)。
A minority of patients without obstruction at rest or on physiologic provocation (about 10%) have progressive end-stage heart failure that is refractory to maximum medical management and may ultimately become candidates for heart transplantation (Fig. 3).
许多此类患者具有独特的表型重塑,转化为收缩泵衰竭(射血分数<50%),通常伴有心室扩大,舒张末期和收缩末期容积增加,以及MRI上弥漫性心肌替代瘢痕引起的肥大消退,瘢痕很可能是微血管缺血所造成。
Many such patients have unique phenotypic remodeling with transformation to systolic pump failure (ejection fraction, <50%), often associated with enlarged ventricular chambers and increased end-diastolic and end-systolic volumes, as well as regression of hypertrophy due to diffuse myocardial replacement scarring on MRI that is probably the result of microvascular ischemia.
约一半的终末期心力衰竭患者在舒张功能障碍的情况下保留了收缩功能,并且心室重塑很少。
About half of patients with end-stage heart failure have preserved systolic function and minimal ventricular remodeling in the presence of diastolic dysfunction.
除了与临界性射血分数相关的广泛纤维化和终末期疾病的家族史之外,很少有因素可预测终末期心力衰竭。
Few factors predict end-stage heart failure, other than extensive fibrosis associated with a borderline ejection fraction and a family history of end-stage disease.
用醛固酮拮抗剂螺内酯治疗并不能减轻症状或瘢痕负担。
Treatment with the aldosterone antagonist spironolactone does not reduce the symptom or scar burden.
随着猝死的减少,晚期心力衰竭的治疗(包括心脏移植)在HCM总体治疗中具有更大的重要性。
With the reduction in sudden deaths, management of advanced heart failure (including heart transplantation) assumes greater importance in overall disease management.
在可供选择的消除心力衰竭的方案中,如果移植是唯一剩余的确定性治疗方案(移植受者的平均年龄,45岁),则此类患者的移植相关生存率与其他心肌病或缺血性心脏病患者的移植生存率相似(根据器官共享联合网络[United Network for Organ Sharing]的数据,在1、5和10年时,生存率分别为85%、75%和61%),在专业的HCM治疗中心,生存率可能较高(在5年时为92%)。
Transplantation, for patients in whom this is the remaining definitive option for abolishing heart failure (average age of transplant recipients, 45 years), is associated with a survival rate that is similar to the rate for transplantation in patients with other cardiomyopathies or ischemic heart disease (i.e., 85%, 75%, and 61%, at 1, 5, and 10 years, respectively, according to data from the United Network for Organ Sharing), with potentially superior survival (92% at 5 years) at centers that specialize in the treatment of HCM.
心脏再同步治疗可以在移植前为一些患者提供相对短期的症状缓解。
Cardiac resynchronization therapy can offer relatively short-term symptomatic relief in some patients before transplantation.
在当前的HCM治疗时代,直接归因于心力衰竭的死亡显然不常见,大多数死亡发生于等待移植的患者,而与HCM无关的充血性心力衰竭患者的死亡率仍然较高。
In the current era of treatment for HCM, death directly attributable to heart failure is distinctly uncommon, with most deaths occurring in patients awaiting transplantation, whereas mortality among patients with congestive heart failure unrelated to HCM remains high.
据报告,在一个治疗中心,对于仔细选择的有重度症状的非梗阻性HCM患者,心尖心肌切除术可作为心脏移植的替代治疗方法。
Apical myectomy has been reported at one center to be an alternative to heart transplantation for carefully selected patients with severe symptoms of nonobstructive HCM.
心房颤动
Atrial Fibrillation
心房颤动是HCM患者中最常见的持久性心律失常,是转诊中心约20%患者的症状(发病年龄通常为50~55岁)(图3)。
Atrial fibrillation is the most common sustained arrhythmia in patients with HCM, accounting for symptoms in about 20% of patients at referral centers (usual age at onset, 50 to 55 years) (Fig. 3).
临床上无症状的发作常见,可用于预测有症状的心房颤动,但卒中风险不确定。
Clinically silent episodes are common and predictive of symptomatic atrial fibrillation but with an uncertain risk of stroke.
伴有左心房扩大和功能障碍的血流动力学负荷条件很可能使患者易发生心房颤动,但未排除原发性心房心肌病的可能性。
Hemodynamic loading conditions with left atrial enlargement and dysfunction probably confer a predisposition to atrial fibrillation, although the possibility of a primary atrial myopathy has not been excluded.
心房颤动的不良后果可能与心房对心室充盈的作用消失有关,特别是当存在明显的左心室肥大和舒张功能障碍时。
Adverse consequences of atrial fibrillation can be related to loss of the atrial contribution to ventricular filling, particularly in the presence of marked left ventricular hypertrophy and diastolic dysfunction.
需要心脏复律的、有症状的心房颤动如果反复、不可预测的发作,通常会损害生活质量,但不会增加猝死或心力衰竭进展的风险。
Repetitive and unpredictable episodes of symptomatic atrial fibrillation requiring cardioversion often impair the quality of life but do not increase the risk of sudden death or progression of heart failure.
使用抗心律失常药(例如胺碘酮、索他洛尔、丙吡胺或多非利特)、导管消融术或迷宫(maze)手术(包括心内切开以阻断电回路)联合心肌切除术,可以降低有症状的心房颤动的发生率。
The frequency of symptomatic atrial fibrillation can be reduced with the use of antiarrhythmic drugs (e.g., amiodarone, sotalol, disopyramide, or dofetilide), catheter ablation, or the maze procedure (involving endocardial incisions that block electrical circuits) combined with myectomy.
从阵发性心房颤动转变为永久性心房颤动相对不常见,25%的患者发生这种情况,充分的心率控制通常与轻度症状或无症状相关。
Transition from paroxysmal to permanent atrial fibrillation is relatively uncommon, occurring in 25% of patients, and with adequate rate control is usually associated with mild or no symptoms.
卒中是心房颤动最重要的后遗症,需要用维生素K拮抗剂或新型口服直接抗凝药预防的阈值较低。
Stroke is the most important sequela of atrial fibrillation, warranting a low threshold for prophylaxis with vitamin K antagonists or novel direct oral agents.
当长期使用抗凝治疗时,栓塞性卒中的风险降低至1/7。
The risk of embolic stroke is reduced by a factor of 7 when anticoagulant therapy is administered for extended periods.
使用现代治疗方案时,HCM患者的房颤相关死亡率<每年1%,几乎所有此类死亡均由未采用预防性抗凝治疗的血栓栓塞引起。
With contemporary treatment initiatives, the rate of death associated with atrial fibrillation in patients with HCM is less than 1% per year, and thromboembolism without prophylactic anticoagulation accounts for virtually all such deaths.
结局
Outcomes
对HCM的早期临床描述包括相当高的死亡率(高达每年6%),这主要反映出当时可选择的治疗方案有限。
Early clinical descriptions of HCM included substantial mortality rates (up to 6% per year), largely reflecting the limited management options available at the time.
笔记:
- available
然而,使用现代治疗策略,有可能明确地改变HCM的临床病程。
However, with contemporary therapeutic strategies, it is possible to definitively alter the clinical course of this disease.
通过使用这些策略,HCM相关死亡率可以低至每年0.5%(代表与35年前的死亡率相比降低90%),死亡率的降低与年龄无关,并且儿童和年轻成人也出现了死亡率降低,而儿童和年轻成人的HCM自然史在传统上最具侵袭性(图4)。
With the use of such strategies, the HCM-related mortality rate can be as low as 0.5% per year (representing a 90% reduction in mortality from 35 years ago), independent of age and including children and young adults, in whom the natural history of the disease has traditionally been the most aggressive (Fig. 4).
笔记:
independent of 与···无关
最近在波士顿塔夫茨医疗中心(Tufts Medical Center)进行的一项研究纳入了1,700例连续登记的HCM患者,161例(9%)患者的生存可以直接归因于治疗方法的重大创新,包括使用植入式除颤器。
In a recent study at Tufts Medical Center, in Boston, involving 1700 consecutively enrolled patients with HCM, survival could be directly attributed to major treatment innovations, including implantable defibrillators, in 161 patients (9%).
笔记:
- survival in xxx patients
事实上,HCM患者中的大多数死亡与HCM无关,非心脏疾病或共存的心脏疾病对生存的威胁最大,特别是在老年患者中。
Indeed, most deaths in affected patients are unrelated to HCM, with noncardiac or coexisting cardiac conditions posing the greatest threat to survival, particularly in older patients.
**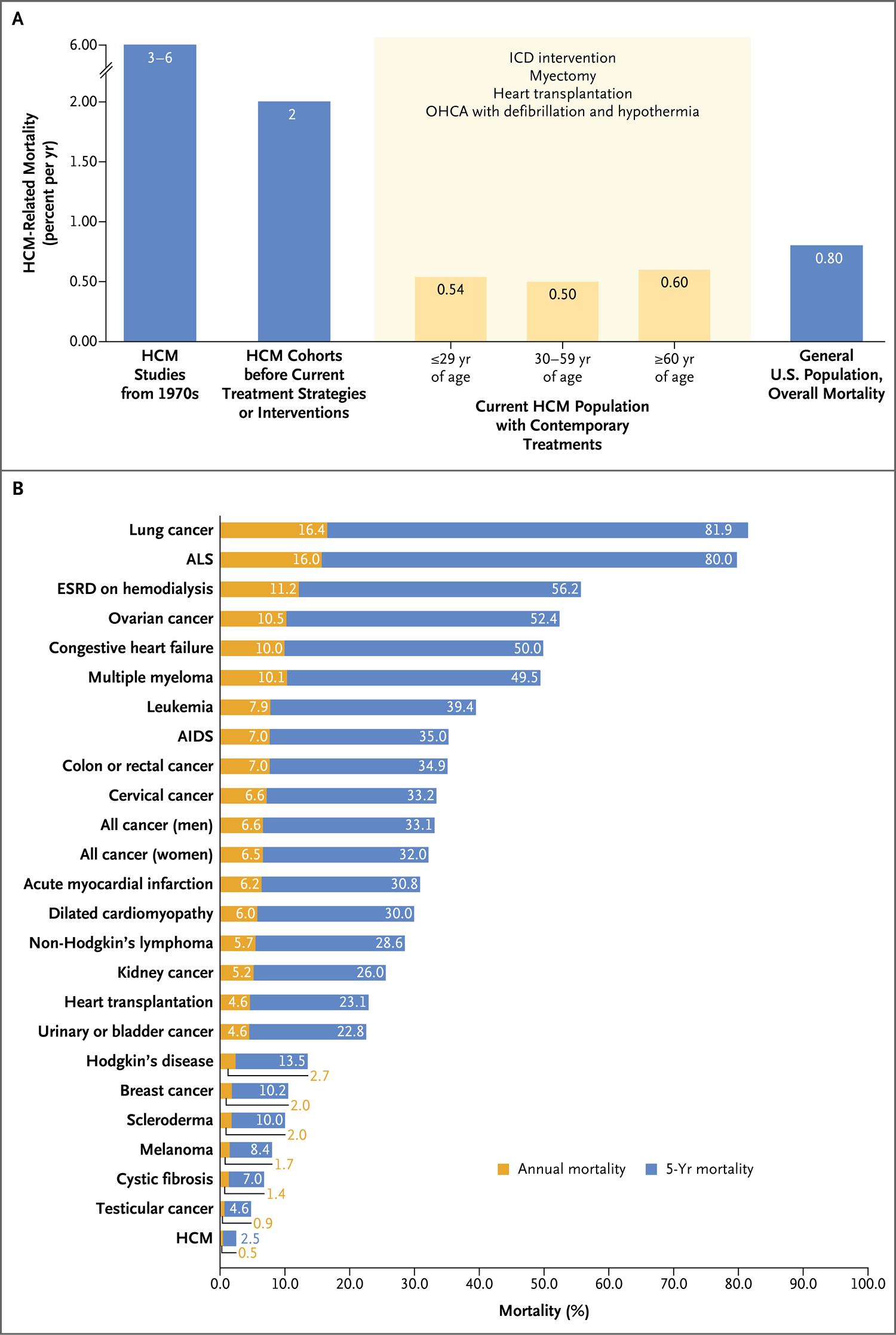
图4. HCM引起的死亡风险
Figure 4 (facing page). Risk of Death Attributable to HCM.
图A显示了超过50年死亡率的下降,涵盖各治疗时代。
Panel A shows the decrease in mortality over a period of more than 50 years, encompassing various treatment eras.
OHCA表示院外心脏停搏。
OHCA denotes out-of-hospital cardiac arrest.
图B显示采用现代治疗时的HCM相关死亡率,并与采用当前治疗的其他疾病的相关死亡率进行比较。
Panel B shows mortality associated with HCM with contemporary treatment, as compared with mortality associated with other disorders with current treatments.
AIDS表示获得性免疫缺陷综合征,ALS表示肌萎缩侧索硬化,ESRD表示终末期肾脏病。
AIDS denotes acquired immunodeficiency syndrome, ALS amyotrophic lateral sclerosis, and ESRD end-stage renal disease.
在特征上,HCM不是一种进行性疾病;在患者一生中,仅10%的HCM患者出现≥2种主要(但可治疗的)并发症。
HCM is not characteristically a progressive disorder; two or more major (but treatable) complications develop in only 10% of affected patients during their lifetime.
总体上,目前主要在多学科专业HCM治疗中心获得了良好治疗结果,这些良好治疗结果代表了使世界许多地区的HCM患者达到治疗平等这一可实现的目标。
Taken together, the favorable treatment results, obtained largely in multidisciplinary centers specializing in the management of HCM, represent an achievable goal for equalizing the disparities in the care of patients with HCM in many parts of the world.
笔记:
- taken together
结论
Conclusions
HCM一度被认为是一种罕见疾病,预后不良,且可选择的治疗方案有限;现在则公认HCM是一种全球性、相对常见且可治疗的遗传性心脏病,通常不会影响预期寿命(图4)。
Once regarded as a rare condition with an ominous prognosis and limited management options, HCM is now recognized as a worldwide, relatively common, and treatable form of genetic heart disease that often does not affect life expectancy (Fig. 4).
笔记:
- life expectancy 预期寿命
- 构句方式表现出了文字重心
HCM的特征在于多样化的临床、遗传和形态学特征,包括心律失常、舒张功能障碍或左心室流出道梗阻导致猝死的风险,这些是进行性心力衰竭的主要决定因素。
The disease is characterized by diverse clinical, genetic, and morphologic features, including a risk of sudden death from arrhythmia, diastolic dysfunction, or left ventricular outflowtract obstruction, which is the major determinant of progressive heart failure.
笔记:
- 包含关系是翻译重点
现代成像技术(包括应用MRI和运动[应激]超声心动图检出静息时不存在的主动脉下压力梯度)和改良的风险分层流程显著改善了临床诊断和治疗。
Clinical diagnosis and treatment have been greatly enhanced by modern imaging techniques (including MRI and exercise [stress] echocardiography to uncover subaortic gradients that are absent at rest) and a refined algorithm for risk stratification.
可用于所有主要并发症的现代治疗策略能够影响HCM的自然史,提供更乐观的HCM治疗前景,治疗方法包括可降低猝死风险的植入式除颤器、对流出道梗阻患者的心力衰竭有永久性逆转作用的心肌切除术(室间隔酒精消融术是心肌切除术的一种可选的替代手术方法)、用于非梗阻性终末期疾病的心脏移植,以及对心房颤动引起的栓塞性卒中有预防作用的抗凝疗法。
Contemporary management strategies that influence the natural history of HCM, which are now available for all major complications, offer a more optimistic view of the disease, with a therapeutic armamentarium that includes implantable defibrillators to reduce the risk of sudden death, surgical myectomy (with alcohol septal ablation as a selective alternative) for permanent reversal of heart failure in patients with outflow obstruction, heart transplantation for patients with nonobstructive end-stage disease, and anticoagulant therapy to prevent embolic stroke caused by atrial fibrillation.
这种治疗模式是由过去20年中的创新临床科学推动,已经将心血管不良事件和死亡风险降低至低于其他心脏疾病或非心脏疾病患者的水平,并因此大幅度延长了HCM患者的预期寿命,提高了HCM患者的生活质量。
This management paradigm, driven by innovative clinical science over the past two decades, has greatly improved life expectancy and the quality of life for patients with HCM by reducing the risks of adverse cardiovascular events and death to levels below the levels among patients with other cardiac or noncardiac disorders.
NEJM的官方中文译文(特指此篇),断句时,更倾向靠拢原文。导致部分句子有些拗口。
作者简介:
四川外国语大学成都学院翻译系英语(翻译方向)专业
重庆医科大学外国语学院英语笔译翻译硕士
英语专业八级
人事部三级、二级英语笔译资格证书持证
人事部三级英语口译资格证书持证
文思海辉技术有限公司 QQ音乐歌词翻译(全职,2014年年度优秀新人)
重庆润泽医药有限公司 医学翻译实习生(翻译、数据整理)
成都创思立信信息技术有限公司 医学翻译(中英翻译、校对、导师)
曾多次为凤凰科技,解放军某高校,成都某化妆品公司提供翻译服务
工作邮箱:wnxcn@foxmail.com